Home / Research Articles / Semaglutide vs Tirzepatide vs Retatrutide: Comparing GLP-1 Receptor Agonists
Semaglutide vs Tirzepatide vs Retatrutide: Comparing GLP-1 Receptor Agonists
Key Takeaways
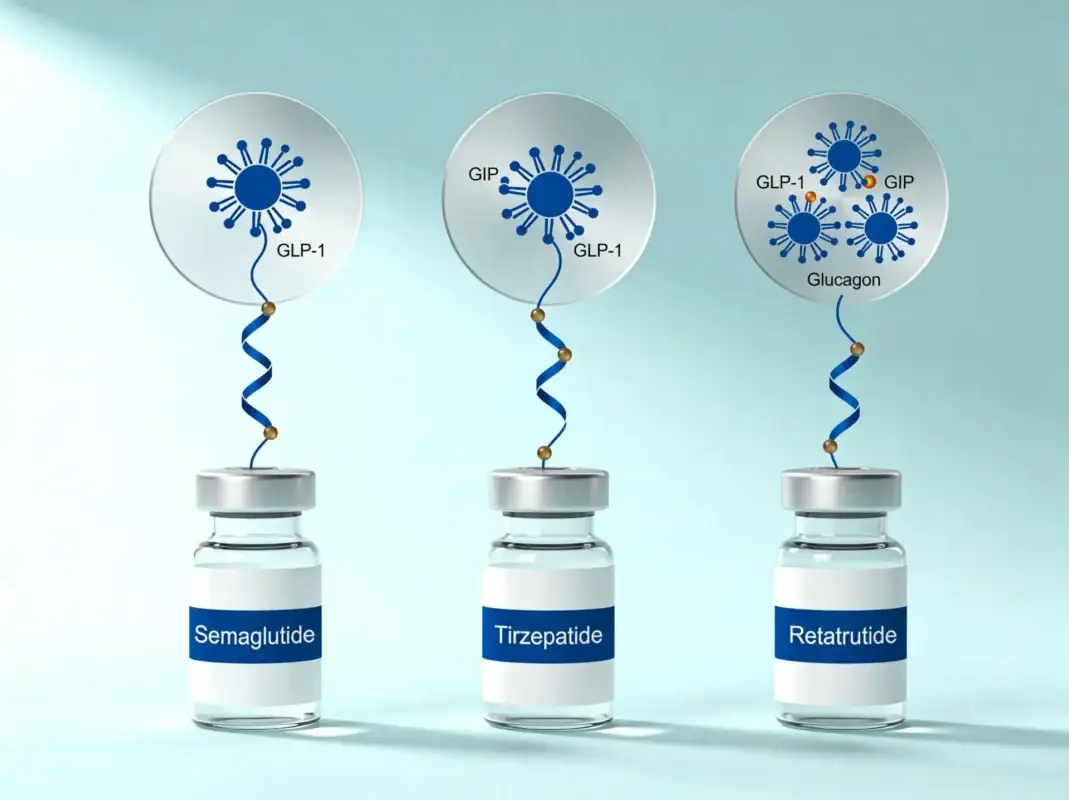
- Semaglutide, Tirzepatide, and Retatrutide represent three successive generations of incretin pharmacology: single, dual, and triple receptor agonism respectively.
- In the SURPASS-2 head-to-head trial, Tirzepatide produced larger HbA1c and weight reductions than Semaglutide; in early phase 2 obesity trials, Retatrutide produced larger weight reductions than eithe
- All three compounds use a fatty-acid-modified, albumin-binding design that extends half-life and supports once-weekly dosing in clinical research.
- Semaglutide and Tirzepatide are approved for human therapeutic use (Ozempic, Wegovy, Rybelsus and Mounjaro, Zepbound); Retatrutide remains investigational.
- The choice between the three compounds for a specific research application depends on which receptor pathways the research question requires.
Researchers comparing Semaglutide, Tirzepatide, and Retatrutide are looking at three successive generations of incretin pharmacology compressed into less than a decade of clinical development. Semaglutide, first published in 2015, activates one receptor. Tirzepatide, first published in 2018, activates two. Retatrutide, first published in 2022, activates three. Each added receptor introduced new mechanistic territory — and each produced measurably larger effects than the compound before it in head-to-head and population-comparable trials.
This article compares Semaglutide, Tirzepatide, and Retatrutide across structure, mechanism, research depth, and the practical question that researchers actually ask: which compound fits which research question.
At-a-Glance Comparison
| Attribute | Semaglutide | Tirzepatide | Retatrutide |
|---|---|---|---|
| Amino acids | 31 | 39 | ~39 |
| Receptor mechanism | GLP-1 agonist | GIP / GLP-1 dual agonist | GIP / GLP-1 / glucagon triple agonist |
| Molecular weight | ~4113 g/mol | ~4814 g/mol | ~4731 g/mol |
| Half-life | ~7 days | ~5 days | ~6 days |
| First published | 2015 (Lau et al.) | 2018 (Coskun et al.) | 2022 (Coskun et al.) |
| Developer | Novo Nordisk | Eli Lilly | Eli Lilly |
| Approval status | Ozempic, Rybelsus, Wegovy | Mounjaro, Zepbound | Investigational only |
| Landmark obesity trial weight reduction | ~15% (STEP 1) | ~20% (SURMOUNT-1) | ~24% (phase 2) |
| Cardiovascular outcomes trial | SELECT (positive) | SUMMIT, SURPASS-CVOT (ongoing/published) | Not yet completed |
How Semaglutide Works
Semaglutide activates the GLP-1 receptor. Native GLP-1 is an incretin hormone secreted by intestinal L cells in response to food intake, with a half-life of one to two minutes before degradation by dipeptidyl peptidase-4 (DPP-4). Semaglutide carries two structural modifications — an Aib substitution at position 8 and a C18 fatty diacid linker at position 26 — that confer DPP-4 resistance and albumin binding, extending the half-life to approximately seven days.
The four primary effects of GLP-1 receptor activation are: glucose-dependent insulin secretion from pancreatic beta cells, glucagon suppression from alpha cells, delayed gastric emptying, and central satiety signaling in the hypothalamus and brainstem. A 2022 review by Drucker in Molecular Metabolism synthesizes the GLP-1 receptor pharmacology in detail [Ref. 6].
For a complete breakdown of Semaglutide’s structure, mechanism, and research applications, see our Semaglutide research deep dive.
How Tirzepatide Works
Tirzepatide activates both the GLP-1 receptor and the GIP (glucose-dependent insulinotropic polypeptide) receptor. The GLP-1 pathway produces the same four effects covered above; the GIP pathway adds several mechanistic threads not present in single-agonist compounds.
The GIP receptor is expressed on adipocytes (where activation influences lipid storage and insulin sensitivity), on bone-forming and bone-resorbing cells (with implications for bone metabolism research), and in the central nervous system (where it contributes to appetite regulation and energy expenditure). When both receptors are activated simultaneously, the insulin response to glucose is amplified beyond what either receptor produces alone.
The clinical relevance of dual agonism was established in the SURPASS-2 trial, published by Frias and colleagues in the New England Journal of Medicine in 2021 [Ref. 1]. Tirzepatide was tested head-to-head against once-weekly Semaglutide 1 mg in subjects with type 2 diabetes, with statistically significant superiority for Tirzepatide across HbA1c reduction and body weight at all three doses tested. SURPASS-2 remains the foundational head-to-head citation in the GLP-1 research literature.
For a complete breakdown of Tirzepatide’s structure and mechanism, see our Tirzepatide research deep dive.
How Retatrutide Works
Retatrutide activates three receptors: GIP, GLP-1, and the glucagon receptor. The first two pathways produce the effects covered for Tirzepatide. The glucagon receptor pathway adds territory neither previous compound covers.
Glucagon receptor activation increases resting energy expenditure through effects on hepatic metabolism, brown adipose tissue, and substrate utilization. The same activation promotes hepatic lipolysis and beta-oxidation, reducing lipid accumulation in the liver — which is why Retatrutide has attracted particular interest in research on metabolic dysfunction-associated steatotic liver disease (MASLD). Importantly, glucagon receptor activation tends to raise blood glucose, which is the opposite of the GLP-1 effect; the balanced design of Retatrutide intentionally uses GLP-1-mediated glucose-lowering to offset glucagon-mediated glucose-raising, producing net glycemic improvement while gaining the metabolic and thermogenic benefits.
In a phase 2 obesity trial published by Jastreboff and colleagues in the New England Journal of Medicine in 2023, Retatrutide produced approximately 24% mean body weight reduction at 48 weeks at the highest dose tested — the largest effect documented in any published GLP-1-class trial to date [Ref. 4].
For a complete breakdown of Retatrutide’s structure and mechanism, see our Retatrutide research deep dive.
Where They Overlap
The three compounds share substantial mechanistic and practical ground.
GLP-1 receptor activation. All three compounds activate the GLP-1 receptor, producing the same baseline set of incretin effects: glucose-dependent insulin secretion, glucagon suppression, delayed gastric emptying, and central satiety signaling.
Extended half-life via albumin binding. All three use a fatty-acid-modified design that binds reversibly to serum albumin, slowing renal clearance and supporting once-weekly dosing in clinical research.
Glycemic and weight effects. Each has been studied in type 2 diabetes and obesity research, with progressively larger effects as the mechanism expands. Wilding 2021 (STEP 1) [Ref. 2], Jastreboff 2022 (SURMOUNT-1) [Ref. 3], and Jastreboff 2023 [Ref. 4] represent the landmark obesity trials for the three compounds respectively.
Lyophilized research formulations. All three are sold as lyophilized powders for laboratory research, reconstituted with bacteriostatic water before use.
Where They Differ
The distinctions matter more than the overlap.
Receptor selectivity. Semaglutide engages one receptor; Tirzepatide engages two; Retatrutide engages three. Each added receptor extends the mechanistic territory the compound can reach. GIP receptor activation (in Tirz and Reta) adds adipose, bone, and central appetite effects. Glucagon receptor activation (in Reta only) adds thermogenesis, hepatic lipid mobilization, and energy expenditure.
Magnitude of weight reduction. In population-comparable phase 2/3 obesity trials, mean weight reductions have escalated with receptor count: approximately 15% (Sema, STEP 1), 20% (Tirz, SURMOUNT-1), 24% (Reta, phase 2). Direct head-to-head data exists only for Sema vs Tirz (SURPASS-2 [Ref. 1], confirming Tirz superiority).
Regulatory status. Semaglutide and Tirzepatide are approved by FDA and Health Canada for human therapeutic use under their brand names. Retatrutide is investigational and has not received regulatory approval anywhere.
Cardiovascular outcomes data. Semaglutide has completed positive cardiovascular outcomes trials in both diabetic (SUSTAIN-6) and non-diabetic obesity populations (SELECT [Ref. 5]). Tirzepatide cardiovascular outcomes data is accumulating through SURPASS-CVOT and SUMMIT. Retatrutide cardiovascular outcomes data is not yet available at scale.
Research breadth. Semaglutide’s research base is the deepest, spanning over a decade of clinical trial data. Tirzepatide’s base is shorter but expanding rapidly since 2022 approval. Retatrutide’s base is the newest, with phase 2 data published in 2023 and phase 3 programs underway.
Choosing Between Them for Specific Research Applications
Practical guidance based on what each compound’s literature actually supports.
Type 2 diabetes glycemic research — Semaglutide has the deepest literature; Tirzepatide produced superior outcomes in the head-to-head SURPASS-2 trial. Either is reasonable depending on the comparator question. Retatrutide phase 2 data also supports use, but the trial base is smaller.
Obesity research — All three are reasonable. Magnitude of effect escalates with receptor count, so the choice depends on whether the research question is about a specific mechanism or about maximum weight effect.
Cardiovascular outcomes research — Semaglutide, with the most complete trial data (SELECT in non-diabetic obesity, SUSTAIN-6 in diabetic populations).
Heart failure with preserved ejection fraction (HFpEF) — Tirzepatide, based on the SUMMIT trial published in 2024.
Steatotic liver disease (MASLD) — Retatrutide, based on its unique glucagon receptor activation. Glucagon receptor agonism directly promotes hepatic lipid mobilization in ways the other two compounds do not.
Bone metabolism research — Tirzepatide or Retatrutide, both of which engage the GIP receptor. Semaglutide does not.
Thermogenesis / energy expenditure research — Retatrutide, with its glucagon receptor activation contributing directly to resting energy expenditure.
Comparative pharmacology research — All three together, designed as a mechanism-escalation series. Researchers can verify reconstitution math for any of them against our peptide reconstitution calculator.
Sourcing Lab-Tested Semaglutide, Tirzepatide, and Retatrutide
All three compounds are heavily counterfeited in the grey-market peptide trade, with mislabeling between them being especially common. Their molecular weights are close enough that visual inspection cannot distinguish them, but distinct enough that mass spectrometry can: 4113 g/mol for Semaglutide, 4814 g/mol for Tirzepatide, 4731 g/mol for Retatrutide.
A credible Certificate of Analysis for any of the three should show HPLC purity expressed as a percentage, mass spectrometry confirmation matching the expected molecular weight for that specific compound, and an explicit distinction between peptide content and peptide mass.
Kinetic Compounds publishes the full Certificate of Analysis for every batch of all three compounds, with all testing performed by Janoshik Analytical. Researchers can review current batch reports on the Semaglutide, Tirzepatide, and Retatrutide product pages. Our broader testing methodology is documented on our lab testing and COA page, and the full GLP-1 and metabolic research peptide catalog lists all related compounds.
For approved pharmaceutical Semaglutide or Tirzepatide intended for human therapeutic use, researchers and clinicians should obtain Ozempic, Wegovy, Rybelsus, Mounjaro, or Zepbound through regular pharmaceutical channels. Research-grade material is not a substitute for these products in any clinical context.
Researching the GLP-1 receptor agonist class? Our complete GLP-1 and metabolic research peptide catalog covers Semaglutide, Tirzepatide, Retatrutide, and related compounds — all independently lab-tested with current Certificates of Analysis available.
Related Peptides
Related peptides will load here via PHP snippet.
Available for Research
Research Tools
Quality Promise
very batch independently tested by Janoshik Analytical. 98% purity minimum.
Frequently Asked Questions
What's the main difference between Semaglutide, Tirzepatide, and Retatrutide?
<p>Semaglutide activates one receptor (GLP-1). Tirzepatide activates two (GIP and GLP-1). Retatrutide activates three (GIP, GLP-1, and glucagon). Each added receptor extends the compound's mechanism into new physiological territory — Tirzepatide adds adipose and bone effects via GIP; Retatrutide adds thermogenesis and hepatic lipid mobilization via glucagon.</p>
Which compound produces the largest weight reduction in research?
<p>In landmark obesity trials, mean weight reductions were approximately 15% for Semaglutide (STEP 1), 20% for Tirzepatide (SURMOUNT-1), and 24% for Retatrutide (phase 2). The progression generally tracks with receptor count.</p>
Which of the three is approved as a medication?
<p>Semaglutide is approved as Ozempic, Wegovy, and Rybelsus. Tirzepatide is approved as Mounjaro and Zepbound. Retatrutide is investigational and has not received regulatory approval. Approval status applies to the pharmaceutical-grade products only — research-grade material in all three cases is intended for laboratory research only.</p>
Can these compounds be combined in research?
<p>Combination protocols across GLP-1-class compounds are not standard in the research literature. Because the three compounds share GLP-1 receptor activity, combining them would produce overlapping rather than complementary mechanisms — quite different from the rationale that justifies, for example, BPC-157 and TB-500 combination protocols where the mechanisms are genuinely distinct.</p>
How are these compounds reconstituted for research?
<p>All three are lyophilized peptides reconstituted with bacteriostatic water. Mass-to-volume math is similar across the three but molar concentrations differ because of the different molecular weights. Our reconstitution calculator handles the conversions automatically.</p>
Are all three legal in Canada?
<p>Semaglutide and Tirzepatide are approved by Health Canada for human therapeutic use as their brand-name products. Research-grade versions of all three (Semaglutide, Tirzepatide, Retatrutide) are legal to purchase and possess in Canada for laboratory research purposes only.</p>
Where can I find Certificates of Analysis for all three?
<p>Kinetic Compounds publishes batch-specific Certificates of Analysis from Janoshik Analytical on each product page. COAs can also be requested directly via research@kineticcompounds.com.</p>
References
- Ref. 1 — Frias JP, Davies MJ, Rosenstock J, et al. (2021). "Tirzepatide versus Semaglutide Once Weekly in Patients with Type 2 Diabetes." New England Journal of Medicine, 385(6):503-515.
- Ref. 2 — Wilding JPH, Batterham RL, Calanna S, et al. (2021). "Once-Weekly Semaglutide in Adults with Overweight or Obesity." New England Journal of Medicine, 384(11):989-1002.
- Ref. 3 — Jastreboff AM, Aronne LJ, Ahmad NN, et al. (2022). "Tirzepatide Once Weekly for the Treatment of Obesity." New England Journal of Medicine, 387(3):205-216.
- Ref. 4 — Jastreboff AM, Kaplan LM, Frías JP, et al. (2023). "Triple-Hormone-Receptor Agonist Retatrutide for Obesity — A Phase 2 Trial." New England Journal of Medicine, 389(6):514-526.
- Ref. 5 — Lincoff AM, Brown-Frandsen K, Colhoun HM, et al. (2023). "Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes." New England Journal of Medicine, 389(24):2221-2232.
- Ref. 6 — Drucker DJ (2022). "GLP-1 physiology informs the pharmacotherapy of obesity." Molecular Metabolism, 57:101351.
Continue Reading
For Research Use Only Products described on this site are intended for laboratory research purposes only. They are not approved by Health Canada for human consumption, diagnosis, treatment, or prevention of any medical condition.