Home / Research Articles / CJC-1295 with DAC vs without DAC: A Research Comparison
CJC-1295 with DAC vs without DAC: A Research Comparison
Key Takeaways
- CJC-1295 with DAC and CJC-1295 without DAC (also called Mod GRF 1-29) are based on the same modified GRF 1-29 peptide sequence — the structural difference is a single C-terminal addition that binds co
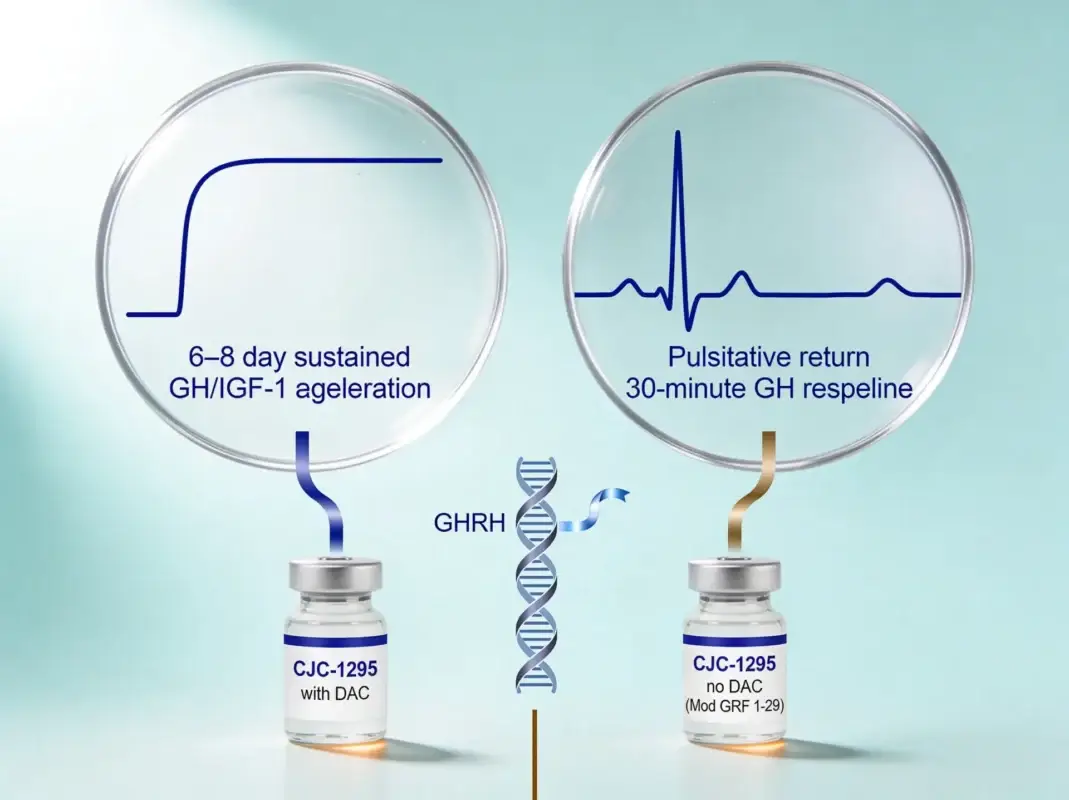
- The DAC modification extends the half-life from approximately 30 minutes (without DAC) to approximately 6–8 days (with DAC) — a roughly 300-fold difference that fundamentally changes the compound's re
- The without-DAC variant produces sharp, transient GH pulses that preserve the natural pulsatile pattern of GH secretion, while the with-DAC variant produces sustained GH and IGF-1 elevation lasting ro
- The choice between variants is dictated by the research question: pulsatile GH dynamics call for without-DAC; sustained GH/IGF-1 elevation calls for with-DAC.
- Both variants act through the same GHRH receptor mechanism and are not approved by any regulatory agency for human therapeutic use.
Researchers comparing the two CJC-1295 variants are looking at one of the most striking examples of pharmacokinetic engineering in modern peptide research. The base peptide — modified GRF 1-29 — has a half-life of approximately 30 minutes. Adding a single covalent modification at the C-terminus that binds serum albumin extends the half-life to approximately 6–8 days. The same fundamental peptide sequence becomes, functionally, two different research compounds.
This article compares CJC-1295 with DAC against CJC-1295 without DAC across structure, pharmacokinetics, research applications, and the practical question that determines which variant fits a given research design. The general background on the CJC-1295 family is covered in our CJC-1295 deep dive; this article focuses specifically on the variant selection question.
At-a-Glance Comparison
| Attribute | CJC-1295 with DAC | CJC-1295 without DAC (Mod GRF 1-29) |
|---|---|---|
| Amino acid sequence | Modified GRF 1-29 + DAC linker | Modified GRF 1-29 only |
| Structural modification | D-Ala, Gln, Ala, Leu substitutions + C-terminal maleimidopropionyl-lysine (DAC) | D-Ala, Gln, Ala, Leu substitutions only |
| Molecular weight | ~3,647 Da | ~3,367 Da |
| Half-life in circulation | ~6–8 days | ~30 minutes |
| GH release pattern | Sustained elevation over days | Sharp transient pulse |
| Natural pulsatility | Altered (sustained activation) | Preserved (acute pulse) |
| Typical research administration | Weekly | Multiple times daily or per session |
| Foundational citation | Teichman et al. 2006 (Ref. 1) | Implied by base GRF 1-29 literature (Ref. 4) |
How Both Variants Work
Both CJC-1295 variants share the same primary mechanism: agonism of the growth hormone-releasing hormone receptor (GHRH-R), a G-protein-coupled receptor expressed primarily on somatotroph cells in the anterior pituitary. Receptor activation triggers a cAMP-mediated signaling cascade that stimulates the synthesis and pulsatile secretion of growth hormone (GH) from the pituitary into systemic circulation.
The downstream effects are also shared: increased GH release, increased hepatic IGF-1 production, and negative feedback regulation via somatostatin and IGF-1 itself. A 2001 review by Veldhuis and Bowers provides comprehensive coverage of the underlying pulsatile GH secretion biology that contextualizes both variants [Ref. 4].
The difference is not in what the variants do at the receptor — both activate the same receptor through the same primary mechanism — but in how long receptor activation persists, and the downstream physiological consequences of that difference.
The DAC Modification
The Drug Affinity Complex (DAC) is the single structural feature that distinguishes the two variants. It is a maleimidopropionyl-lysine residue added at the C-terminus of the modified GRF 1-29 sequence. The maleimide group reacts covalently with free cysteine residues — and the most abundant free-cysteine-bearing protein in human circulation is serum albumin, present at approximately 35–50 g/L in adult plasma.
When CJC-1295 with DAC enters circulation, the maleimide group forms a covalent bond with albumin’s free Cys34 residue. The peptide is now tethered to a large circulating protein with a half-life of approximately 21 days. This dramatically slows renal clearance (the kidneys cannot filter albumin-sized molecules efficiently), and the result is an effective peptide half-life of approximately 6–8 days — roughly 300 times longer than the without-DAC variant’s 30 minutes.
Without DAC, the modified GRF 1-29 sequence has no albumin-binding capacity. It circulates as a free peptide and is cleared rapidly by renal filtration and enzymatic degradation, producing the 30-minute half-life characteristic of the unmodified base sequence.
The structural difference is small (one C-terminal addition). The pharmacokinetic difference is enormous. This is the essential insight of the DAC platform.
Pulsatile vs Sustained GH Release
The pharmacokinetic difference between the two variants produces qualitatively different patterns of growth hormone release, and these patterns drive most of the research design implications.
Without DAC: Pulsatile GH release
The without-DAC variant produces a sharp, transient GH pulse with a clear onset and clearance within hours. After administration, GH levels rise rapidly, peak within roughly 30–60 minutes, and return toward baseline within 2–4 hours. This pattern closely mimics the natural pulsatile pattern of physiological GHRH-driven GH secretion, which produces discrete pulses every 3–4 hours under basal conditions with the largest endogenous pulses during slow-wave sleep [Ref. 4].
Research designs that study pulsatile GH responses, acute GH dynamics, or sleep-architecture-correlated GH pulses generally use the without-DAC variant. The compound is well-suited to protocol designs that administer the peptide at specific time points and measure GH responses across discrete windows.
With DAC: Sustained GH/IGF-1 elevation
The with-DAC variant produces sustained elevation of both GH and IGF-1 over days rather than hours. The foundational paper by Teichman and colleagues in 2006 in the Journal of Clinical Endocrinology and Metabolism documented this profile in detail: after a single dose of CJC-1295 with DAC, serum GH and IGF-1 remained elevated above baseline for approximately one week, with peak IGF-1 elevation around days 4–7 post-administration [Ref. 1].
An important nuance documented in a 2006 follow-up paper by Ionescu and Frohman: although CJC-1295 with DAC produces sustained elevation of mean GH levels, the underlying somatotroph pulsatility is preserved [Ref. 2]. The somatotroph cells continue to release GH in discrete pulses; the sustained GHRH stimulation simply raises the baseline from which those pulses occur, producing higher mean levels without flattening the pulse architecture entirely.
A 2004 paper by Bowers and colleagues in JCEM used a 30-day continuous subcutaneous infusion model to study the same general phenomenon with a GHRP-2 secretagogue, demonstrating that sustained upstream stimulation produces persistent GH and IGF-1 elevation without complete loss of pulsatility — a finding that helps contextualize the CJC-1295 with DAC pharmacokinetic profile [Ref. 5].
A 2018 review by Sigalos and Pastuszak synthesizes the broader literature on this class of compounds and their distinct pharmacokinetic profiles [Ref. 3].
Which Variant for Which Research Question
Practical guidance based on what the variants’ respective profiles actually support.
Acute pulsatile GH dynamics research — Without DAC. The 30-minute half-life produces discrete pulses that can be measured against baseline. Multiple-administration protocols within a session are feasible.
Sustained GH/IGF-1 elevation research — With DAC. The 6–8 day half-life supports weekly dosing with continuous elevation across the dosing interval. Useful for studying chronic effects of elevated GH/IGF-1 exposure.
Sleep-architecture-correlated GH research — Without DAC. Preserves the natural pulsatile pattern, allowing study of compound-induced pulses against the natural sleep-driven endogenous pulse cycle.
Body composition research (chronic exposure) — With DAC. Sustained GH/IGF-1 elevation over weeks is the relevant exposure profile for most body composition research designs.
Combination protocols with Ipamorelin — Either variant. Both can be combined with Ipamorelin (which acts on the ghrelin receptor, a separate upstream pathway). Without-DAC + Ipamorelin protocols study acute synergy; with-DAC + Ipamorelin protocols study sustained baseline GH elevation with acute Ipamorelin pulses layered on top. The combination protocol research framework is covered in our CJC-1295 + Ipamorelin combination protocol article.
Comparison to Tesamorelin — Without DAC is closer to Tesamorelin in pharmacokinetic profile (Tesamorelin half-life ~26–38 minutes), while with DAC is much longer-acting than any approved GHRH analog. Researchers comparing GHRH-axis approaches to other modalities often select based on whether the research question calls for short-acting or long-acting pharmacokinetics.
Frequency of administration logistics — Without DAC requires more frequent administration (daily, sometimes multiple times daily); with DAC supports weekly administration. For long-running protocols, this is a meaningful logistical consideration.
Sourcing Lab-Tested CJC-1295 Variants
CJC-1295 mislabeling between the two variants is one of the most common quality issues in the growth hormone peptide research market. Independent testing data from grey-market suppliers regularly reveals products labeled “CJC-1295 with DAC” that actually contain the without-DAC form, products labeled “Mod GRF 1-29” that contain the with-DAC variant, and products labeled simply “CJC-1295” with no indication of which variant the vial actually contains.
The two variants are distinct molecules with different molecular weights: approximately 3,647 Da for with DAC, approximately 3,367 Da for without DAC. The 280 Da difference is small enough that visual inspection cannot distinguish them, but distinct enough that mass spectrometry can. A credible Certificate of Analysis for either variant should specify which form the vial contains, with mass spectrometry confirmation matching the expected molecular weight for that specific variant.
Kinetic Compounds sells both variants as separate products, each with its own Certificate of Analysis specifying the form. The with-DAC product is documented on the CJC-1295 product page, and the without-DAC form is on the CJC-1295 no DAC product page. All batches are tested by Janoshik Analytical, and current batch reports are published on each product page. Our broader testing methodology is documented on our lab testing and COA page, and the principles of reading a peptide COA are covered in our reading a Certificate of Analysis article.
For researchers working across the full GHRH analog class, our growth hormone research peptide catalog lists both CJC-1295 variants alongside related compounds including Ipamorelin and Tesamorelin.
Researching the GHRH-axis peptide class? Our complete growth hormone research peptide catalog covers both CJC-1295 variants, Ipamorelin, Tesamorelin, and related compounds — all independently lab-tested with current Certificates of Analysis available on each product page.
Related Peptides
Related peptides will load here via PHP snippet.
Available for Research
Research Tools
Quality Promise
very batch independently tested by Janoshik Analytical. 98% purity minimum.
Frequently Asked Questions
What does "DAC" stand for in CJC-1295?
<p>DAC stands for Drug Affinity Complex, a maleimidopropionyl-lysine residue added at the C-terminus of the modified GRF 1-29 peptide sequence. The maleimide group binds covalently to free cysteine residues on serum albumin, tethering the peptide to a long-circulating protein and dramatically extending the functional half-life.</p>
Is CJC-1295 without DAC the same as Mod GRF 1-29?
<p>Yes. CJC-1295 without DAC and Mod GRF 1-29 are two names for the same compound — the modified GRF 1-29 sequence with the D-Ala, Gln, Ala, and Leu substitutions, but without the DAC modification. The naming inconsistency in the research market is one reason mislabeling between variants is so common.</p>
Why does the DAC modification extend the half-life so much?
<p>Free peptides are cleared rapidly by renal filtration and enzymatic degradation. When the DAC modification binds the peptide to serum albumin, the peptide is now physically attached to a protein that is too large to be filtered efficiently by the kidneys and that has a much longer circulating half-life of its own (~21 days). The peptide's clearance becomes coupled to albumin's clearance, producing the ~300-fold half-life extension.</p>
Can the with-DAC variant be used for acute research?
<p>Yes, but with caveats. The with-DAC variant does produce GH/IGF-1 elevation acutely after dosing, but the sustained elevation across days means any acute measurement window is overlaid on a continuously elevated background. For research questions that specifically require acute, transient GH pulses against a clean baseline, the without-DAC variant is the better tool.</p>
Can the without-DAC variant be used for sustained research?
<p>Sustained GH/IGF-1 elevation is difficult to achieve with the without-DAC variant because of the 30-minute half-life — even repeated daily dosing produces a series of pulses rather than continuous elevation. For research designs that require sustained exposure, the with-DAC variant is the appropriate tool.</p>
Are either variant approved as a medication?
<p>No. Neither CJC-1295 variant has been approved by FDA, Health Canada, EMA, or any other regulatory agency for human therapeutic use. Both are intended exclusively for laboratory research. The only approved compound in the GHRH analog class is Tesamorelin, which is structurally distinct from CJC-1295.</p>
Where can I find Certificates of Analysis for both variants?
<p>Kinetic Compounds publishes batch-specific Certificates of Analysis from Janoshik Analytical on each variant's product page. The COA specifies which variant the vial contains, with mass spectrometry confirming the molecular weight matches the labeled variant. COAs can also be requested directly via research@kineticcompounds.com.</p>
References
- Ref. 1 — Teichman SL, Neale A, Lawrence B, Gagnon C, Castaigne JP, Frohman LA (2006). "Prolonged stimulation of growth hormone (GH) and insulin-like growth factor I secretion by CJC-1295, a long-acting analog of GH-releasing hormone, in healthy adults." Journal of Clinical Endocrinology and Metaboli
- Ref. 2 — Ionescu M, Frohman LA (2006). "Pulsatile secretion of growth hormone (GH) persists during continuous stimulation by CJC-1295, a long-acting GH-releasing hormone analog." Journal of Clinical Endocrinology and Metabolism, 91(12):4792-4797.
- Ref. 3 — Sigalos JT, Pastuszak AW (2018). "The Safety and Efficacy of Growth Hormone Secretagogues." Sexual Medicine Reviews, 6(1):45-53.
- Ref. 4 — Veldhuis JD, Bowers CY (2001). "Neurophysiological regulation and target-tissue impact of pulsatile growth hormone secretion in the human." Growth Hormone & IGF Research, 11 Suppl A:S25-37.
- Ref. 5 — Bowers CY, Granda R, Mohan S, Kuipers J, Baylink D, Veldhuis JD (2004). "Sustained elevation of pulsatile growth hormone (GH) secretion and insulin-like growth factor I (IGF-I), IGF-binding protein-3 (IGFBP-3), and IGFBP-5 concentrations during 30-day continuous subcutaneous infusion of GH-
Continue Reading
For Research Use Only Products described on this site are intended for laboratory research purposes only. They are not approved by Health Canada for human consumption, diagnosis, treatment, or prevention of any medical condition.